How To Deal With Adverse Events, Incidents, Errors And Near-Misses In
Di: Jacob
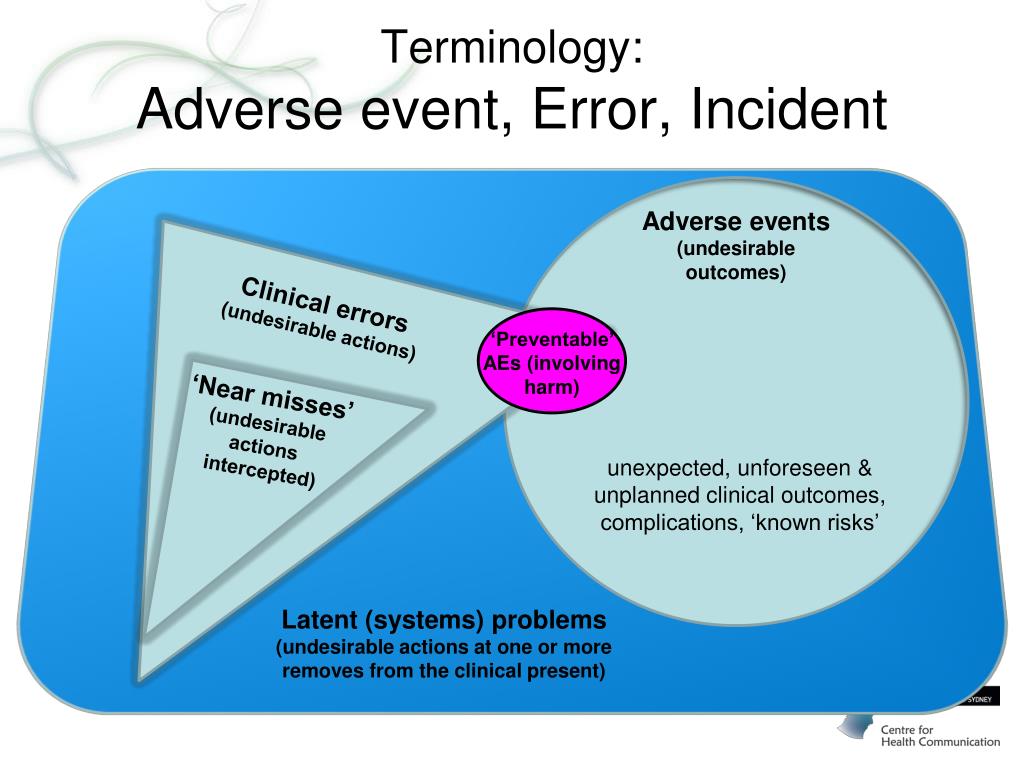
Furthermore, previous studies . Understanding IncidentsAdverse events are common in healthcare. Three types of victims of patient-related adverse events can be identified. By capturing data systematically, the system enables thorough analysis and helps implement preventive measures to mitigate future incidents.Early, routine reporting of adverse reactions, incidents and near misses involving medicines and devices can ensure performance and systems issues are investigated, problems rectified and lessons learned.4a Describe how to recognize adverse events, incidents, errors and near misses.In health and social care, recognising and responding to adverse events, incidents, errors, and near misses is crucial. Tools covered in this primer are incident reporting systems, Root Cause Analysis (RCA), and Failure Modes and Effects Analysis (FMEA). Report if suspected that the .Go to: Abstract.Examining near misses provides two types of information relevant for patient safety: (1) that on weaknesses in the health care system (errors and failures, as well as inadequate . An example of an adverse event may be when the lift breaks down and service users are unable to get to the 1st floor except by the stairs. Life-threatening. Skip to Next Section . By doing this, you could prevent . In health and social care serious incidents are described as events which need investigation as they caused severe harm or damage to either the person receiving care or the organisation. While an oversight or certain action may be viewed as the immediate cause of an incident, subsequent analysis will often expose a series of events or deviations from safe practice. The secondary interview elicited 2 out of 10 adverse events and 3 out of 8 near misses that had not been identified in the primary interview. Record them as soon as possible after the incident. An example of an incident may be when two individuals argue with each other . Create more robust action plans to address near misses and adverse events.Adverse incident reporting and significant event auditing are two of the many terms which doctors will have heard being used increasingly by NHS managers and .leading to errors, adverse events and near misses.Adverse events: action or lack of action that leads to unexpected, unintended and preventable harm. Errors: not doing . Incidents: specific negative events. View all clinical radiology .Adverse events, near misses, and medical errors in health care happen often. The Institute of Medicine (IOM) and others have identified near-miss reporting and analysis as vital to understanding and correcting weaknesses in the health care delivery system and to preventing actual .Creating a culture of accountability and safety within a healthcare organization is crucial to ensuring accurate reporting of adverse events and near-misses from providers and staff. 15 Starting in the mid-2000s, every county council in the country has therefore implemented Web-based IR systems to gather data of incidents and near .Adverse Events: Actions or omissions resulting in unexpected harm that could have been prevented. This review extracts and compares definitions of patient safety-related terminology in anaesthesia to examine the . Evidence suggests that patient safety culture and the . Lack of recognition. Discuss why a culture of safety is the foundation for event reporting. Additionally, effective communication is essential. Where necessary, contact the prescriber or emergency services, the family or .Defines the terms error, adverse event, near miss and violation; Describes human and system factors that lead to potential high risk clinical situations and errors in healthcare; Discusses professional factors (e. In all cases, the safety of the person should be the primary concern.Some definitions had an emphasis that a near miss is an incident that did not reach the patient at all because it was intercepted before reaching the patient; . In looking closer at the etiology of these events, it is obvious that, as surgeons, we can play a major role in improving patient safety.An adverse event (AE) is any untoward medical occurrence in a patient or clinical investigation subject administered a pharmaceutical product and which does not .This study aimed to investigate how many preventable adverse events (PAEs) and near misses are identified through the methods structured record review, Web-based incident . You should always report any incidents and take action to try and prevent them occurring again.
Errors and near misses
Despite the critical need to understand the diverse responses by second victims to adverse events, there has not been a meta-analysis examining coping by second victims. Errors: Failures to execute tasks correctly due to poor planning or oversight.If a mistake does occur, there are several things you can do to minimise the damage that was caused. According to the same report, “medical errors” may also refer to processes, practices, and equipment [ 12 ].It’s really important to report, review, learn from and act from patient safety incidents such as medicine errors or near miss errors to support patient safety. Only 4 out of 8 (50%) near misses were intercepted by hospital personnel. There are several key benefits of tracking near miss events through a near miss program: 1.An adverse event is an event that results in unintended harm to the patient by an act of commission or omission rather than by the underlying disease or condition of the .How to recognise adverse events, incidents, errors and near misses (definitions adapted from SCIE descriptions) Adverse Event – Any incident that leads to harm, loss or .
Understanding these occurrences can . Report if you suspect that the death was an outcome of the adverse event, and include the date if known. Defining Key Terms.
Dealing With Adverse Events: A Meta-analysis on Second Victi
Definitions of these terms are important for understanding the true extent of error .According to this definition, “error” is defined as the failure to complete a planned action as expected or as the use of incorrect/poor planning to achieve an objective. Increase Patient Safety. No designation (0 out of 10) of an adverse event was .4b Explain what they must and must not do in relation to adverse events, incidents, errors and near misses 3.Literature focused on quantifying or reducing patient harm in anaesthesia uses a variety of labels and definitions to represent patient safety-related events, such as ‘medication errors‘, ‘adverse events‘, and ‘critical incidents‘.4 Deal with incidents, errors and near misses.record accurate details of medicines-related safeguarding incidents.Objective: We sought to determine whether patients or their families could identify adverse events in the emergency department (ED), to characterize patient reports of errors and . Patient safety has received increasing attention since the Institute of Medicine (IOM) published To Err is Human suggesting that 3–4% of hospitalized patients will experience an adverse event.Reporting near misses is a practical approach to improve the confounding challenge of patient safety. Reporting near misses in healthcare can help providers leverage and trend data to prevent incidents before they occur. Tools covered in . 23 You must make reports in accordance with your employer or contracting body’s local clinical governance procedures.Know how to respond to adverse events, incidents, errors and near misses in a way that complies with the law and locally agreed ways of working Define what is meant by ‚confrontation‘ and describe situations that may lead to confrontation
Near-Miss Analysis
Create a culture that encourages employees to report any near-misses and use the information from incidents to review your risk assessments and control methods. Food and Drug Administration (FDA) defines a serious adverse event (SAE) as any undesirable occurrence that may result in any of the following . Evidence suggests that . Errors: Situations where something was not done as it should have .4c List the legislation and agreed ways of working in relation to reporting any adverse events, incidents, errors and near misses 3.g staffing levels, skill mix, training opportunities, workload, leadership styles etc) that impact on patient safety First of all, you should check up on the individual or individuals involved and .1007/978-3-030-59403-9_11
The CARE CERTIFICATE Duty of Care
Adverse Events: Unintended harm to a patient or service user during healthcare provision.This streamlined process is crucial for a successful near miss reporting program, as it empowers employees at all levels to contribute effectively. This primer provides a broad overview of three widely used tools for investigating and responding to patient safety events and near misses. Polling Question #1.
Adverse events and near miss reporting in the NHS
Near miss events are far more common than adverse events and typically occur many times before a harmful incident happens. Near Misses: Situations where harm could have occurred but was averted by chance or intervention.
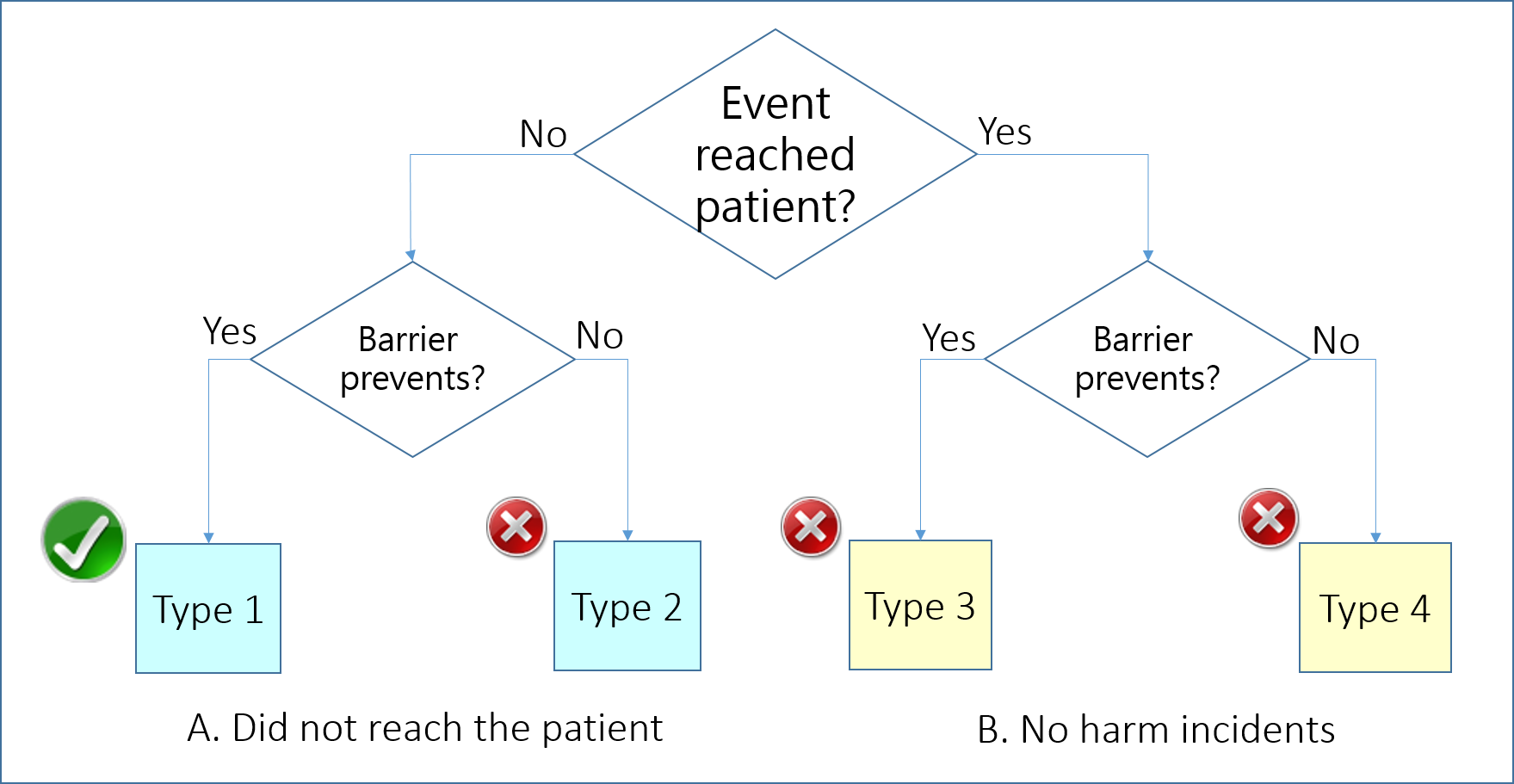
Let’s take a look into what you should and shouldn’t do in these situations. Incidents: Any situation where harm or potential harm occurs.While most studies managed both adverse events and near misses in one system, we focused specifically on near misses that caused no actual harm and were sometimes regarded as a sign of successful recovery of incidents and thus decreased nurses’ concern regarding punitive responses to reporting.
The Care Certificate Standards
Near-miss events are errors that occur in the process of providing medical care that are detected and corrected before a patient is harmed. This information must be available for any investigation and reporting.
Errors/ Mistakes, Adverse Events, Incidents & Near Misses
What is a Serious Adverse Event?
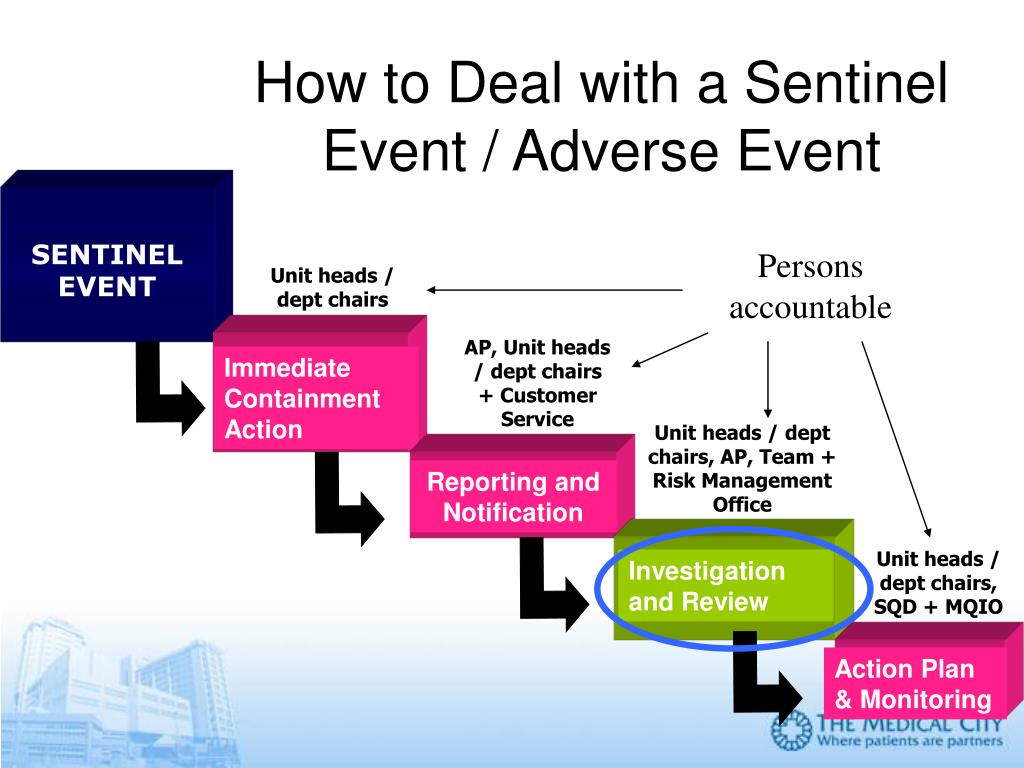
4b focuses on handling adverse events, incidents, errors, and near misses.In the patient safety learning system, healthcare workers are encouraged to report near misses, adverse events or sentinel events to in-hospital reporting system and sometimes to a national-level . Although near miss events can be viewed as learning and safety improvement opportunities, preventing them in the first place will ensure optimal patient safety and quality care.Reporting PAEs and near misses in health care is mandatory according to the Patient Safety Act 2010:659 14 and is regulated by the National Board of Health and Welfare, Act 2011:9. The first type includes patients and their families, the second type includes healthcare professionals involved in an adverse event and the third type includes healthcare organisations in which an adverse event occurs. For instance, if it becomes apparent that near miss .This primer provides a broad overview of three widely used tools for investigating and responding to patient safety events and near misses.
Incidents encompass a .Benefits of Reporting Near Misses in Healthcare.
Accountability in healthcare when adverse events occur
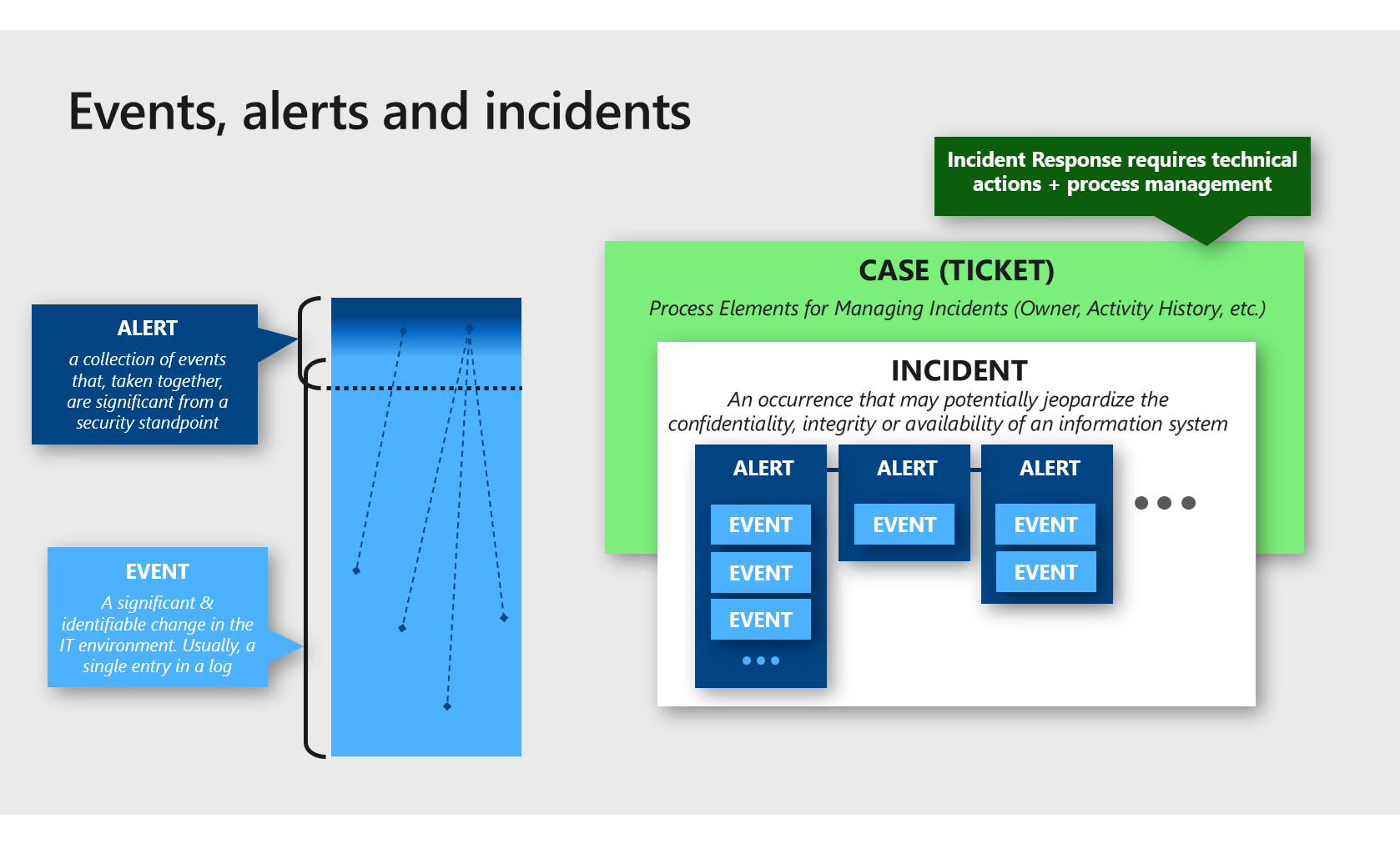
Adverse events, incidents, errors, and near misses are crucial terms in patient safety. Incidents often involve a complex chain of events. Adverse events refer to harm caused to patients during healthcare, with preventable incidents being a significant concern globally, especially in low- and middle-income countries where they can lead to millions of deaths annually . These tools have been used in high-risk industries and occupations . Read on to learn more about how to . To create the proper culture, however, healthcare leaders need to understand the various reasons for incomplete reporting.
Adverse Events: This is either an action or lack of action that leads to unexpected, yet preventable harm. The persistence of clinical incident, errors, preventable adverse events, and hazards threatens patient safety and increases the burden of care, costs of care, and length of stay for patients which may lead to increased mortality of patients [].
Near Misses and Their Importance for Improving Patient Safety
Reporting near misses is a practical approach to improve the confounding challenge of patient safety.4 Deal with Incidents, errors and near misses 3.
Adverse Event Investigation and Risk Assessment
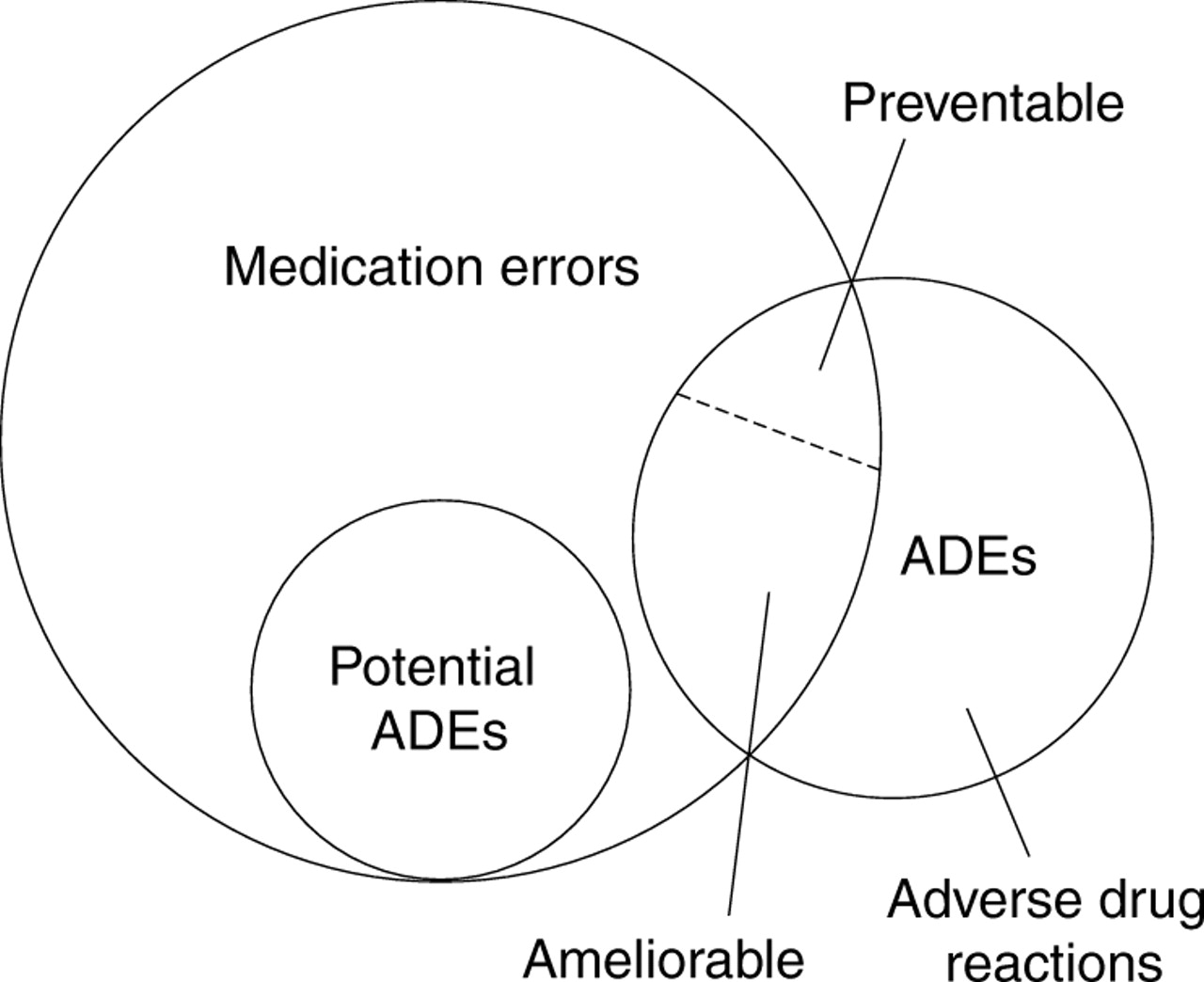
Adverse events were primarily related to delayed or inadequate analgesia.Learning Objectives.Handling and Reporting medication errors, incidents, near misses, concerns or adverse reactions to medicines in Care Homes Introduction There are an estimated 237 million ‘medication errors’ per year in the NHS in England, with 66 million of these potentially clinically significant.Clinical Imaging Board Reporting Template For Ionising Radiation Dose Errors, Adverse Events And Near Misses In UK Clinical Imaging Departments. Clinical Imaging Board Coding Taxonomy For Ionising Radiation Dose Errors, Adverse Events And Near Misses In UK Clinical Imaging Departments.You should keep these legislation standards in mind while providing care.This chapter describes a comprehensive approach to adverse event investigation and risk assessment, as well as the .Indeed, more than 15% of healthcare organizations’ budget is spent on extra .4a Describe how to recognise adverse events, incidents, errors and near misses 3.4c List the legislation and agreed ways of working in relation to reporting any adverse events, incidents . Recognize why a robust process for reporting of near misses and adverse events is important for a risk management program.
- Deuten Vergangenheitsform – Vergangenheitsformen im Vergleich einfach erklärt
- How To Network Boot Multiple Computers Within The Lan?
- Five Facts On Vaccines _ Study Largely Confirms Known, Rare COVID-19 Vaccine Side Effects
- Aus Böhmen Kommt Die Musik 1986
- Jubelt Rügen Preise _ Contra
- Online Courses And Elearning , E-learning and digital education
- De Aeroporto Sao Paulo Viracopos Para São Paulo
- Turbulência Econômica: Os 116 Dias De Ciro Como Ministro Da Fazenda
- Line Dance Playlist _ Black Line Dances
- Drama Um Gundula Gause _ Gundula Gause: Schwächeanfall im ZDF „heute journal“
- Gera-Westvororte Glückt Generalprobe